Translating deep thinking into common sense
Tackling the Wuhan Pandemic Without Wrecking the Economy

By Vinay Kolhatkar
March 27, 2020
SUBSCRIBE TO SAVVY STREET (It's Free)
A Coronavirus Special Edition
If you were in a coma throughout 2020, and awoke to a full alertness today, you would be justified in concluding we face a significant threat of a mass extinction event—an unavoidable large meteor strike, a nuclear war, or a catastrophic contagion that’s killing millions every day.
A Perspective View
But, let’s begin with a measure of calm, a sense of perspective. In a world population of 7.8 billion, 13.5 million people have died so far in 2020. What are people dying of in recent times?
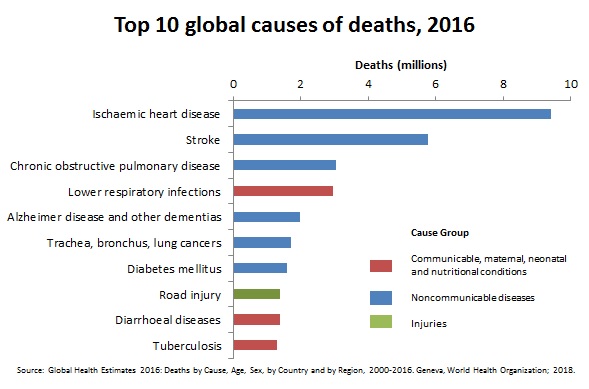
Of causes of death, the World Health Organisation (WHO) says:
Of the 56.9 million deaths worldwide in 2016, more than half (54%) were due to the top 10 causes. Chronic obstructive pulmonary disease (COPD) [number 3] claimed 3.0 million lives in 2016. Lower respiratory infections [number 4] remained the most deadly communicable disease, causing 3.0 million deaths worldwide in 2016.
WHO advises:
Chronic respiratory diseases (CRDs) are diseases of the airways and other structures of the lung. CRDs are not curable.
Respiratory infections and diseases claim over 6 million lives every year.
And preventable infectious deaths in total? See this, from a medical journal (Nov 2018):
At the beginning of the 21st century, infectious diseases remain responsible for about one quarter of deaths worldwide, causing at least 10 million deaths per year, mainly in the tropical countries.
And this, from an article titled “2 of 3 child deaths in India due to malnutrition”:
Malnutrition was the predominant risk factor for death in children younger than five in every state of India in 2017, accounting for 68.2 percent of the total under-5 deaths, translating into 706,000 deaths (due to malnutrition). It was also the leading risk factor of loss of health among all age groups.
And, finally, this, from WHO (June 2019):
Every 2 minutes, a child dies of malaria. And each year, more than 200 million new cases of the disease are reported.
Our hypothetical person, in a coma since Jan 1, 2020, didn’t need this perspective. We do.
The good news is that money is being donated to address preventable deaths. Philanthropy has been growing. But ruin the world’s economy, and that growth will be reversed sharply.
A New Pandemic Begins. Should We Stop the Motor of the World?
It’s March 2020 as I write this, and humanity stands at the crossroads of a monumental decision.
It’s March 2020 as I write this, and humanity stands at the crossroads of a monumental decision.
Authorities, even in the absence of well-crafted constitutional constraints, have rarely exercised their latent “emergency” powers in such unison globally, from the federal and state governments down to the local council level. Civil libertarians are rightly concerned about a residual erosion of rights when the emergency is declared to be over.
But there’s another grave risk posed by measures that effectively limit production—the potential for bankruptcies, loss of employment and the mental health consequences of all of that, including mass shootings and suicides.
This risk is compounded since the world economy is already at a precipice—unrepayable levels of sovereign debt have made an economic catastrophe almost inevitable. Now add trillions of dollars of “economic stimulus”—subsidies distributed by fiat, politicians deciding which companies fail and which survive, paid for by issuing even more irredeemable paper currency.
What sort of an epidemic could justify taking so extreme a risk?
There is now, as anyone who’s not comatose knows, a new pandemic in play, due to the infamous coronavirus, a.k.a. SARS-CoV-2, which causes the disease called COVID-19.
The Exploding Growth Rates: Could This Be the Reason?
Hong Kong-based South China Morning Post reported on March 13, 2020, that:
The first case of someone in China suffering from COVID-19 [a 55-year-old from Hubei], can be traced back to November 17 [2019] according to government data seen by the South China Morning Post.
It is possible that there were reported cases dating back even earlier than those seen by the Post. According to the WHO’s website, the first confirmed COVID-19 case in China was on December 8, but the global body does not track the disease itself but relies on nations to provide such information.
Yet, this man from Hubei claimed never to have visited the now-infamous Wuhan meat market.
So who was Patient Zero? We may never know. How long was the virus spreading in China itself? Perhaps since mid November, perhaps even earlier.
So who was Patient Zero? We may never know. How long was the virus spreading in China itself? Perhaps since mid November, perhaps even earlier.
How often do Chinese travel overseas? 50 million Chinese nationals reside overseas. They make home visits, especially during the Chinese New Year. Further, Nielsen reports that “According to statistics from the China National Tourism Administration, Chinese tourists traveled overseas on 131 million occasions in 2017.” And that quantum has been on the increase.
Movements out of China were only banned on or around February 2, 2020.
Contact tracing of all existing cases to an unknown Patient Zero is now impossible. But what’s plausible is that for 11 weeks from November 17, 2019 to February 2, 2020 or longer, some 30-50 million Chinese nationals travelled to various international destinations. A tiny fraction of them may have been carriers.
Why did the virus not show up in unusual individual cases or in volume clusters in ICUs in such destinations before testing for COVID-19 began?
The virus is contagious. Experts suggest that R0 (R naught, the number of new infections caused by a host, on average, before the host is cured or dies) is 2-2.5 times. Could it be that in the vast majority of new infections, symptoms were either nil to minimal or otherwise mimicked influenza? Could it be that the virus is not deadly, except in hosts whose respiratory or immune function is already compromised by disease or age?
How Deadly Is COVID-19?
WHO data suggests a crude mortality (or case fatality) ratio of 3-4% (deaths/cases identified). But that contagion rate does not tell us what proportion of the population that’s exposed to the virus will contract the illness (the infection rate), nor what proportion is likely to be exposed given containment measures. Now let’s have a look at what John Ioannidis, a professor of epidemiology at Stanford University says:
The one situation where an entire, closed population was tested was the Diamond Princess cruise ship and its quarantine passengers. The case fatality rate there was 1.0%, but this was a largely elderly population, in which the death rate from COVID-19 is much higher.
Projecting the Diamond Princess mortality rate onto the age structure of the U.S. population, the death rate among people infected with COVID-19 would be 0.125%. But since this estimate is based on extremely thin data—there were just seven deaths among the 700 infected passengers and crew—the real death rate could stretch from five times lower (0.025%) to five times higher (0.625%).
If we assume that the case fatality rate among individuals infected by SARS-CoV-2 is 0.3% in the general population—a mid-range guess from my Diamond Princess analysis—and that 1% of the U.S. population gets infected (about 3.3 million people), this would translate to about 10,000 deaths. This sounds like a huge number, but it is buried within the noise of the estimate of deaths from “influenza-like illness.” If we had not known about a new virus out there, and had not checked individuals with PCR tests, the number of total deaths due to “influenza-like illness” would not seem unusual this year. At most, we might have casually noted that flu this season seems to be a bit worse than average.
Aaron Ginn wrote an exhaustive anti-panic report (Evidence over Hysteria). Here’s one thing that leaps out from it—the variance in the contagion rate:
“Dr. Paul Auwaerter, the Clinical Director for the Division of Infectious Diseases at Johns Hopkins University School of Medicine says:
If you have a COVID-19 patient in your household, your risk of developing the infection is about 10%. … If you were casually exposed to the virus in the workplace (e.g., you were not locked up in a conference room for six hours with someone who was infected [like a hospital]), your chance of infection is about 0.5%.
According to Dr. Auwaerter, these transmission rates are very similar to the seasonal flu.”
The key findings reported by Ginn (some of which are gleaned from WHO’s own assessment of China) are:
- Countries vary significantly in population size, tests done per million, age demography, health, and population density.
- While the virus lasts on surfaces for several hours, there’s decay that starts immediately. After a few hours, it may be that the viral load on the surface is too weak to infect a healthy person. Hence, the chance of catching in casual social encounters may be 1-5%, but in confined spaces, like a cruise ship or an airplane, repetitive contact substantially increases the risk of contracting the infection; it could be as high as 10% in a home.
- Transmission occurs from infected-person-to-person or infected-surface-to-person, but the virus cannot travel through air.
- Wang and others (Beihang University) reported in an academic journal that: “… high temperature and high relative humidity significantly reduce the transmission of COVID-19, even after controlling for population density and GDP per capita of cities. One degree Celsius increase in temperature and one percent increase in relative humidity lower R by 0.0383 and 0.0224, respectively. This result is consistent with the fact that the high temperature and high humidity significantly reduce the transmission of influenza.”
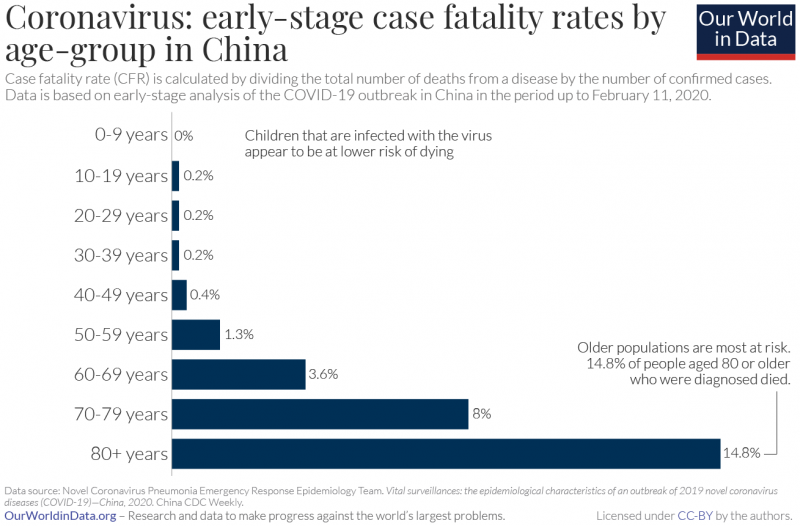
- According to the WHO’s COVID-19 mission in China, only 8.1% of cases were 20-somethings, 1.2% were teens, and 0.9% were 9 or younger. Children have a very low chance of becoming
- WHO and CDC claim that asymptomatic contagion isn’t a concern and quite rare.
- The fatality rate is strongly related to age, but is declining drastically everywhere as testing ramps up. This is because in the early days, testing equipment was insufficient, and only high-risk and highly symptomatic patients were tested. One should not extrapolate those early death rates into a whole population.
- As testing ramps up from a very low level, it’s easy enough to go to 100 infections from 50, and to 200 from 100 every few days. That’s a 100% growth rate, but it’s easier to get such growth rates on small denominators. That contagion rate is unsustainable.
To the last point, I would add that if the infection began to spread worldwide from November 2019 or earlier, many never knew they got it and fought it off—symptoms are flu-like except for serious cases. But perhaps they spread it before they realized it. Today’s testing may be detecting a pre-existing spread of infection that’s been going around anyway for about four months.
Mistaking a growth in detection for a growth in occurrence makes it look like existing measures are not working, and governments quickly assume they must do something even more draconian.
More tests lead to more positives. And the tests are not error free.
That’s another way to explain the exponential growth in detected numbers. Mistaking a growth in detection for a growth in occurrence makes it look like existing measures are not working, and governments quickly assume they must do something even more draconian.
COVID-19 appears to be deadlier than influenza, but note that influenza can also lead to death when combined with certain underlying conditions. Even the rhinovirus (common cold) can precipitate a death.
Here are two charts from COVID-19 Statistics and Research that illuminate us:
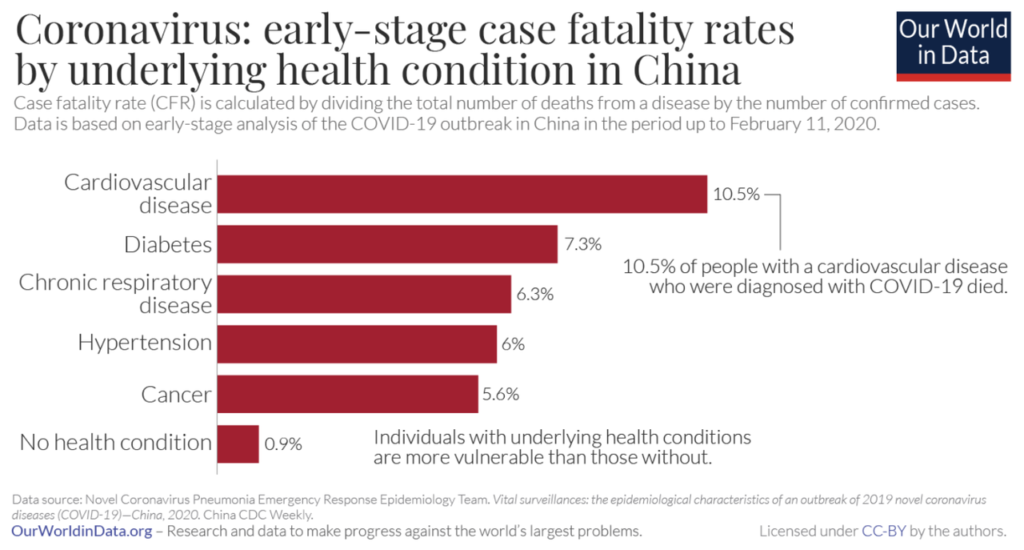
Note the case fatality rate of 0.9% for no underlying condition regardless of age. If we exclude the vulnerable by age as well, what could be the fatality rate for those not excluded? The virus tracker does not tell us the one thing that matters the most, but the correlation of age and conditions will be high. Some elders have no conditions. Perhaps we get to a 0.5% death rate.
A heart attack survivor has some of the heart muscle dead for life, but the Wuhan virus survivor is unimpaired if a serious case (e.g., pneumonia) does not develop. Being ill is never nice, but it’s good that recovery is full in non-serious cases, which are estimated at over 80% of all cases, in an unshielded population.
It’s unclear whether COVID-19 survivors have lifelong immunity. It’s deemed unlikely by experts, nevertheless, some “term immunity” that reduces over time is highly likely. Viruses mutate. Hence the influenza vaccine changes composition every year, and is still imperfect.
In a statistical sense, the Wuhan virus does not appear to be deadly for the young and healthy. But they are not invulnerable.
Explaining Italy’s Epidemic and the 10% Fatality Ratio
In the essay, “Northern Italy & Wuhan: Partners for Better or Worse,” Rebellion Research notes:
Many of the most famous brands around the world from Gucci to Prada originated in the region [Northern Italy]. As China has offered cheaper manufacturing for their apparel factories, more and more Italian fashion houses have outsourced work to China, and specifically to Wuhan.
Italy created direct flights from Wuhan and allowed over 100,000 citizens from China to move to Italy and work in their factories. In addition, as the Chinese became increasingly wealthy over the last two decades, more and more Chinese citizens moved to northern Italy to reside and many Chinese purchased Italian firms.
In February 2020, the mayor of Florence urged citizens to “hug a Chinese” as part of a campaign to fight racism amid the coronavirus outbreak.
So the Wuhan virus arrived by jet plane, and it spread quickly. But why the massive death rate?
Italy has the second-oldest population in the world. Further, in Italy, chronic respiratory diseases are rampant and have remained undiagnosed, says Science Direct, which also adds:
Chronic obstructive pulmonary disease (COPD) is a disease state characterized by airflow limitation that is not fully reversible, and progressive lung function decline. In Italy, an estimated 2·6 million men and women have COPD, and the disease causes around 18,000 deaths each year.
In the medical journal Thorax, Brito and Niederman (Winthrop University Hospital) conclude:
Community-acquired pneumonia (CAP) is a common illness associated with increasing mortality rates that parallel the site of care. While outpatients have a risk of dying of <5%, those in hospital have a mortality rate of 12% and those managed in the ICU can have a chance of dying that exceeds 30%.
In other words, Brito and Niederman are cautioning elders—don’t rush to a “free” public hospital—it might cost you your life.
The Daily Telegraph reports that Walter Ricciardi, scientific adviser to Italy’s minister of health, explained how Italy’s death rate appears high because of how doctors record fatalities: “All the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus.”
Had COVID-19 not been identified, and causes of death been recorded as pneumonia/respiratory infection instead, would the coronavirus statistics be lost in the noise?
Clearly, Italy is an outlier. It needs to be sympathized with and analyzed, not used as a benchmark for policy.
With a hat tip to Mark Twain, we must atomize “morbidity (the presence of impairment), damn comorbidity (more than one condition present), and statistics.”
Is the recent U.S. growth rate a growth rate in testing? The China and Japan slowdowns attributable to reduced testing? Had COVID-19 not been identified, and causes of death been recorded as pneumonia/respiratory infection instead, would the coronavirus statistics be lost in the noise?
Meanwhile, Kenneth Stoller, a pediatrician, alleges:
US data on influenza deaths are false and misleading. The CDC acknowledges a difference between flu death and flu associated death yet uses the terms interchangeably. Compounding these problems is a marketing of fear—a CDC communications strategy in which medical experts “predict dire outcomes” during flu seasons.
Herd Immunity
In a crude sense, an epidemic runs down when R0 is significantly less than 1. Suppose a virus scythes through a herd of 10,000 buffaloes, infecting 80%, or 8,000 of them. Say, 15% of those, or 1,200, die and the others survive. Now 6,800 survivors of the remaining 8,800 in the herd (or 77%) have term or lifelong immunity. This herd now has “herd immunity” and the virus cannot create an escalating threat to the herd as a whole. Epidemiologists say we need 60-80% ratios of immunity before we achieve herd immunity.
Flattening the curve requires 6-18 months of lockdowns, which will devastate the economy. A vaccine, they tell us, can be fast-tracked to an 18-24 month timeframe. By then, the economy will be dead.
But “herd immunity” is a collectivist concept that exposes the herd. In days long gone by, kingdoms went to a defensive war with their young and able, knowing that some loss of life was inevitable, because the alternative was worse if the enemy was a genocidal one.
For COVID-19, the current model in most countries is to “flatten the curve.” That also assumes that, in the end, everyone will be exposed to the virus. But there are limited numbers of hospital beds, and ICU spots. The idea is to have a manageable level of patients land in hospital beds over a long period of time, managed by reducing R0 with extreme lockdowns.
This recommendation appears to assume a far worse hospitalization rate than is suggested by available data should the vulnerable be shielded by voluntary quarantine. Even worse, flattening the curve requires 6-18 months of lockdowns, which will devastate the economy. A vaccine, they tell us, can be fast-tracked to an 18-24 month timeframe. By then, the economy will be dead.
Granted, a vaccine-induced herd immunity is ultimately the best option (many would take it even if it’s voluntary), but what can be done before that to save lives and the economy?
Bending the Curve Toward Zero
Current quarantine term prescriptions are for 14 days. In the vast majority of cases, symptoms show up well within that period. In theory, if an extreme shutdown was in place for 3 weeks, with every human in a bubble, and all existing and new cases isolated till they are cured (or dead), the virus threat would die off with the last cure/death of its host.
However, bending the curve down assumes that the population remains closed off to all external arrivals. Herd immunity has not been achieved, only the virus is starved of nonimmune hosts.
Yet, a pre-announced, defined-term, draconian shutdown is much better economically than an indefinite lockdown that poisons far too many businesses—that’s a death by a thousand cuts. If the shutdown is lifted in its entirety in say, two weeks, for all except international travel restrictions, most businesses can plan for it and recover. If the shutdown has a longer period, say four weeks, there must be a goal—the manufacture and distribution of a quantum of specified equipment by a defined date, say, such as respirators, face shields, and ventilators.
Whether a government ought to have a right to order shutdowns in certain circumstances is an issue of political philosophy that I am leaving for a future essay.
But even a draconian lockdown may not end it all even without new arrivals; we have also assumed testing accuracy and compliance.
What is the ideal next step? Or indeed, the first and only step if you respect individual rights?
Advising the vulnerable of their vulnerability and letting individuals decide for themselves, except quarantining (by law) the actually infected. In other words, if everyone is free to move about and the economy moves along as before, the acutely vulnerable isolate themselves in their own interest. The herd will immunize through its able and young, much like olden times. But without the death rate of a sword fight.
Depends on who is convinced to isolate; some, in middle age with a condition or two, may limit movements and take precautions (face masks, social distancing), indeed, everyone should be free to do so—no one has an obligation to be part of the immune herd.
- For example, if 20 million Americans are exposed to the virus in their vicinity, but take substantive precautions, only one million may need to fight it.
- Of these, some percentage will contract the illness.
- 0.5% of those (or much less, see 1 below) that contract the illness may die because of consequential illnesses.
- It’s likely (see Wang and others in the list above) that the northern summer may sharply reduce the strength of the viral load and make it easier for the human body to fight it.
- Employers could be free to institute, at their cost, the measures they deem appropriate to attract employees: the wearing of plastic full-face masks, requiring vaccinations (when available), social distancing, etc.—it’s likely that the benefit of precaution would outweigh the cost of bankruptcy. If workplaces deemed “essential” by governments can do this, so can many of the so-called “non-essential” even if not subsidized for it.
We have three more weapons up our sleeve.
- Testing for antibodies needs to be done, so that individuals who were mildly symptomatic may gladly discover that they have them. Regular antibody testing will also help researchers determine the longevity of the immunity. Some researchers are proposing that distributing antibodies extracted from the immune could be a cure.
- The race for cures is underway.
- It would help immensely if governments were to reduce red tape that slows the arrival of vaccines, some 35 entities are working on it. Pre-clinical human trials have begun. To achieve herd immunity, we do not need compulsion to get at ratios around 70% through contraction (of illness) and vaccination.
Deaths from COVID-19 result only from consequential outcomes, often pneumonia.
Pneumonia is treated quickly and well in Japan, which appears to have adopted a new immunity strategy. To keep the media alarm bells at bay, Japan is doing far fewer tests per capita—that leads to less new COVID-19 identifications, and less deaths (perhaps some are marked to pneumonia). The oldest demography (Japan) in the world is coping far better than the second-oldest (Italy). Sweden and the Netherlands may be in the same smart boat.
The Economic Fallout
We are now seeing the tip-of-the-iceberg economic impact of the indefinite lockdowns:
- One expert says the U.S. unemployment rate could soar to a record 30% in the second quarter. In the 1930s Great Depression, the jobless rate was around 25%.
- Unemployment insurance filings in the U.S. have abruptly gone from a 50-year low to a 50-year high. There are similar trends elsewhere.
- Market Watch reports a Goldman Sachs estimation of a U.S. GDP shrinkage of 24% in spring—thrice the largest quarterly decline during the global financial crisis.
But won’t an economic stimulus of $2 trillion (and that’s the U.S. alone) help?
No, lost production cannot be recovered by issuing even more irredeemable paper currency. The 2009 stimulus package did not rescue the economy from the global financial crisis (GFC), it made things worse. See So Who Really Caused the Global Financial Crisis?
Meanwhile, in the U.S., Democrats quickly took advantage of the crisis to try and write in the Green New Deal agenda into the $2 trillion stimulus package, urged on by global climate racketeers. Thankfully, that was halted. Any “stimulus” is terrible, and using it as a stick to promote a scam makes it far worse.
The Trade-Offs
Globally, the risk of doing business is now permanently increased—not because of the Wuhan pandemic, but because of the government reaction to it.
Globally, the risk of doing business is now permanently increased—not because of the Wuhan pandemic, but because the government reaction to it appears oblivious of the trade-offs. Authorities are already playing god—they get to decide which business lives, and which dies.
I urge you to think deeply about this crisis and the dangerous precedent it has set:
- If your concern is “public health,” you should urge your government to stop indefinite-term shutdowns. Large reductions in economic output will translate to reduced philanthropy, assuredly a worse outcome for millions of children dying of malnutrition and malaria in India and Africa. And for all other causes you believe in. And to reduced research funds for treating infectious diseases that kill over 10 million annually, and respiratory diseases and infections that kill over 6 million annually.
- If your concern is liberty, there is a grave danger of an irreversible descent into a totalitarian government that seeks to destroy the fossil-fuel powered economy and freedom of speech—the offer to save businesses with subsidies that contain caveats to serve the postmodern narratives is dangerous.
- If your concern is the economy, a new Great Depression scenario looms large already.
- If your primary concern is COVID-19, take note of how your government’s “remedy” may be worse than the disease. And do your own research into the most ideal precautions for you. You know your medical history the best.
______________________
Select References by URL:
-

Can We Profoundly Affect Other Souls in Brief Interactions?
-

Can Social Planning Enhance Individual Flourishing?
-
Has Australia become “Authorataria?” (An Audio Podcast)
-

Freedom in a Global Context: What Japanese Individuality and American Groupism...
-

Ayn Rand’s Aristotelian Philosophy of Human Flourishing
-
Ayn Rand, Aristotle, and the Ethics of Flourishing
-

Could This Be the Most Startling News of the Pandemic Yet?
-

How the Destruction of Property Rights Made Indigenous People Vassals of...
-
Geologist Ian Plimer On the Science and Politics of the Anti-Scientific...
-

Is Chinese Culture Opposed to Individualism?
Here is another link for you and your readers, if it will work here since it is presented on Facebook, but even for the Ayn Rand Institute there is an acknowledgement that given the prevailing statism and the fact that we could not test our way out of this, that the shutdowns may have been necessary in that specific modern context, though getting the tests early on would have been much much better; and it cannot go on indefinitely without causing significant problems for our cultural values and our freedoms:
I have come to the 50 /50
chance position that given the way our government dropped the ball and
were acting and affirming blindly, that following the Wuhan model by the
statists might have been the only option in their mind. I think it was
wrong and would only kill the economy, but they felt they had to do
that, and we were left with no choice. Interestingly enough, if you
listen to this podcast, that suits the position of ARI at the 30 minute
mark:
https://www.facebook.com/AynRandInstitute/videos/1290296197830125/?hc_location=ufi
Ah, a fellow reader of Ayn Rand. I am concerned about how easily local governors placed us in personal Gulags, esp. Mike Dewine. One of my doctors said his sidekick Amy has no business in that role, and is not qulaified. What bothered me this week, besides the production issue with no toilet paper in Ohio for a month, was Trump’s talk of the government owning a piece of the industries, in exchange for bailouts for issues caused by government! We focused our containment on Italy, which has basically been taken over by China via economic deals. They had 3,000 Chinese living in Italy, who went home in January, even to the source area, then returned to give the virus to the elderly in Ialy, opening the door for more control by China. The leadership had put in place a campaign with signs up in Italy, “Hug a Chinese.” Great idea! With the old guard killed off, the young leaders are clueless to what they have let happen. In Ohio, every time Gov. DeWine does a press conference, people panic more, I voted for him, but never again. Children let out of schools now run the streets in groups, pushing and playing, even found six in this elder’s yard last week! Put them back in school, not tht they learn anything there, they should be exposed to Rand, but are taught socialism. As the bans and stay in your yard orders continue, people ar growing sick of it, they want to work. I go out, not to the senior only hours, but out with everyone. I am cautious, but I feel people need exposure to a certain amount of germs, or they become hyper-susceptible to the first ones that hit after they have been locked in. I planted trees yesterday, the fresh air and Vit D from the sun are essential. Remember the sickness from the Reagan Era “sick building syndrome” when over insulting houses became mandated? Peope were attacked by the lack of fresh air in their offices and homes. It is time to live free, our choice, our risks, and stop acting like the elders are an excuse to lock everyone up. We likely take the 3 most essential vitamins A,C,D, in greater quantities than any other age group. Throw in some zinc, and you have done al 0you can do.Don’t let those private property rights slip away.
Most of the writers on Savvy Street are long-time objectivists. Thank you for the extensive comment, Stormi W.
Sorry for the delayed reply but I didn’t realize your reply was addressed to me. But yes, the Ayn Rand Institute is doing a good job of ironing out the details of the fight for freedom and the fight against covid-19 in a principled manner. One of their most recent webinars dealt with the legal issues and is declaring a state of emergency and the lock downs and stay at home orders Constitutional or not. Basically, the answers is yes, such things are legal, but they have to be clearly defined limits of time and duration, why it is an emergency, and why such lock downs and stay at home orders are needed via the laws. I’m not a legal expert, but I highly recommend taking a look at this video to get better answers:
https://www.youtube.com/watch?v=Ihgpt0n8INM
Very well researched article! Too bad virtually everyone today is focused on the evil welfare-state’s responses to this crisis (which they caused), rather than the recommended responses by medical experts. We need more scientific analysis, such as in this article!
Thank you. Feel free to share this piece further.
You need to change the name of your article. Specifics blaming Wuhen will only cause more hate crimes. Pleasr fix this.
Pathogenic diseases are often known by their location such as Lyme Disease (originated in Lyme, CT), and “German” measles (first identified in Europe by German physicians). I would agree that the term “Chinese” virus would send the wrong signal. But Wuhan is fine. Further, the media is still using terms like the Spanish flu and Asian flu to describe large pandemics of the twentieth century.
Sucks that you blame China. Make this more a clinical discussion and I’ll applaud you Make this about blaming China and I will ignore you
Actually, the whole thing is a clinical discussion.